Case Identification
Case ID Number
Tumor Type
Body region
Periosteal reaction
Benign or Malignant
Clinical case information
Case presentation
The patient is a generally healthy 38-year-old licensed practice nurse who has had pain in the left hip which began one year ago. The pain is somewhat lessened by wearing compression tights over the area.
Radiological findings:
The patient is a cigarette smoker and is taking Percocet for the pain. There is no abdominal mass or tenderness. On the left side of the pelvis, there is a palpable mass just inside the anterior superior iliac spine that is mildly tender. There is a fullness in the hip musculature above the trochanter. There is a full range of motion of the hip but there is pain with motion. Distally, the neurovascular status is normal. Sensation is normal in the foot. Circulation is normal.
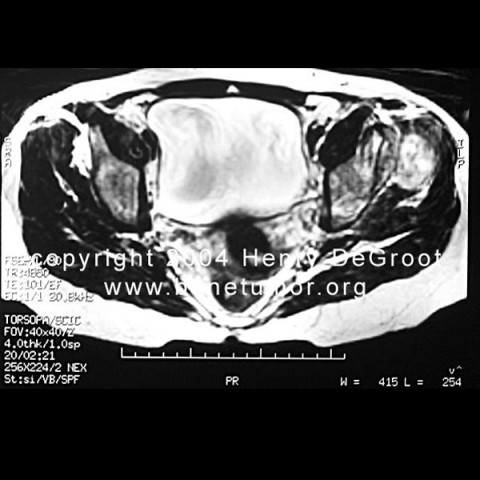
Plain radiographs a vague, lytic, permeative process in the left ilium, with a vague but non-mineralized mass in the soft tissues surrouning the anterior superior iliac spine. n MRI is available for review. There is an abnormality in the left hemipelvis with a intraosseous and extra osseous mass arising from the ileum, with abnormal signal in the ileum from the anterior superior iliac spine all the way down to the supra-acetabular area at the top of the hip joint. There is a soft tissue mass both on the inside and on the outside of the pelvis, it measures at least eight or 10 cm in maximum dimension. There is diffuse abnormality in the hip abductor musculature. The hip joint does not appear to be grossly involved, but the coronal images of the acetabulum show that the lesion reaches down to the subchondral bone of the acetabulum were possibly to be cartilage of the acetabulum on the left side. No definite abnormality is seen within the femoral head or inside the joint itself.
A CT scan of the pelvis shows a partially lytic and destructive mass inside and outside the pelvis with no distinctive mineralization within the soft tissue mass. The tumor appears to arise from the left ileum, just posterior and distal to the anterior superior iliac spine.
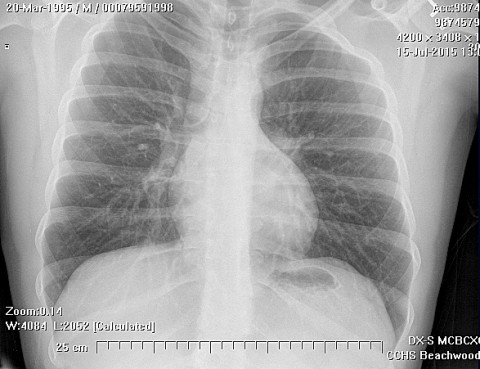
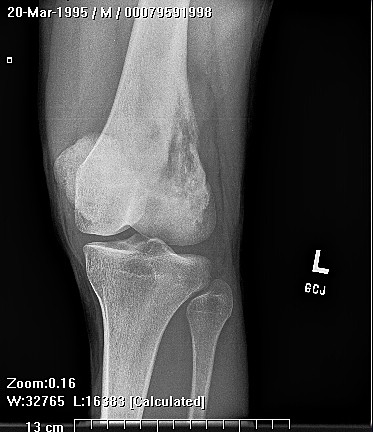
On the bone scan, there is abnormality in the left hemipelvis. There is also slightly increased uptake in the left proximal femur. A CT scan of the chest shows no nodules, no lymphadenopathy, and no evidence of metastasis.
Plain radiographs a vague, lytic, permeative process in the left ilium, with a vague but non-mineralized mass in the soft tissues surrouning the anterior superior iliac spine. n MRI is available for review. There is an abnormality in the left hemipelvis with a intraosseous and extra osseous mass arising from the ileum, with abnormal signal in the ileum from the anterior superior iliac spine all the way down to the supra-acetabular area at the top of the hip joint. There is a soft tissue mass both on the inside and on the outside of the pelvis, it measures at least eight or 10 cm in maximum dimension. There is diffuse abnormality in the hip abductor musculature. The hip joint does not appear to be grossly involved, but the coronal images of the acetabulum show that the lesion reaches down to the subchondral bone of the acetabulum were possibly to be cartilage of the acetabulum on the left side. No definite abnormality is seen within the femoral head or inside the joint itself.
A CT scan of the pelvis shows a partially lytic and destructive mass inside and outside the pelvis with no distinctive mineralization within the soft tissue mass. The tumor appears to arise from the left ileum, just posterior and distal to the anterior superior iliac spine.
On the bone scan, there is abnormality in the left hemipelvis. There is also slightly increased uptake in the left proximal femur. A CT scan of the chest shows no nodules, no lymphadenopathy, and no evidence of metastasis.
Pathology results:
The patient underwent incisional biopsy.
On medium power, the is an irregular pattern of cells. Some of the matrix is blue stained, characteristic of proteoglycans, which make up chondroid matrix, but other areas of dense pink matrix show osteoid production. A higher power view shows the lacy pink osteoid and highlights the variability of the nuclei, which is termed "nuclear atypia" and "nuclear pleomorphism".
On medium power, the is an irregular pattern of cells. Some of the matrix is blue stained, characteristic of proteoglycans, which make up chondroid matrix, but other areas of dense pink matrix show osteoid production. A higher power view shows the lacy pink osteoid and highlights the variability of the nuclei, which is termed "nuclear atypia" and "nuclear pleomorphism".
Special Features of this Case:
Questions for self-study: Construct a differential diagnosis for this lesion. If this lesion is a sarcoma, what surgical option would you recommend for this patient? What choice for reconstruction would you choose? What is the significance of the bone scan uptake in the left proximal femur, and what would you do about it?
Imagen
Case ID Number
Image Types
Image modality
Tumor Name
Tumor Type
Benign or Malignant
Body region
Bone name
Location in the bone
periosteal reaction
position within the bone
Tumor behavior
Tumor density