Case Identification
Case ID Number
Tumor Type
Body region
Benign or Malignant
Clinical case information
Case presentation
This 42 year old healthy man had insidious onset of left groin and hip pain. The pain got so severe he was admitted to the hospital for tests and treatments, but no diagnosis could be made and the pain got worse. The patient decided to go home and find a different doctor.
Radiological findings:
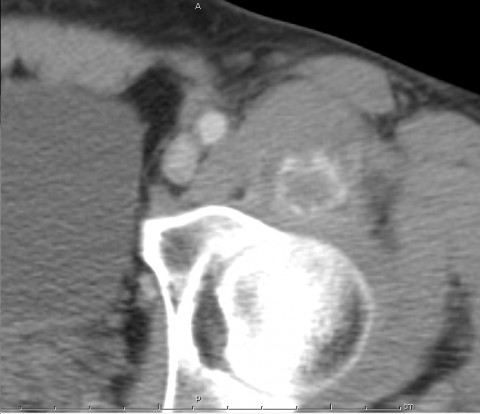
A CT scan with IV contrast (done 10 days before the pt presented) shows contrast collection in an area in the left iliopsoas. There is faint calcification within the substance of the muscle.
An MRI (done 10 days before the pt presented) shows extreme abnormality of the ileopsoas with what appears to be a small collection, calcification, or phlegmon within the iliacus muscle. There is no definite fluid collection. However, the MRI had been intended to be an arthrogram of the hip with contrast injection of the joint done just prior to the examination. It was uncertain based on the interpretation of the radiologist whether the changes were due to extravasation of the contrast material or due to the patient's pathology.
A follow-up computed tomography scan of the pelvis was made when the patient presented. The findings were similar to those in the previous CT scan. There was more definite calcification within the substance of the muscle with a ring that like area of calcification surrounding an unclassified area.
CT scan guided aspiration of the area of the potential collection or calcified muscle was made and there was no fluid. Cultures showed no growth after five days. The radiologist performing the procedure noted that there was palpable calcification within the muscle.
A follow-up magnetic resonance imaging scan of the pelvis was made four days later, this time with no injection of contrast material. This MRI showed that the findings on the previous MRI we are due to the patient's pathology and not due to extravasation of contrast material. The findings were similar in extent to the previous MRI with no significant improvement nor any significant worsening.
An MRI (done 10 days before the pt presented) shows extreme abnormality of the ileopsoas with what appears to be a small collection, calcification, or phlegmon within the iliacus muscle. There is no definite fluid collection. However, the MRI had been intended to be an arthrogram of the hip with contrast injection of the joint done just prior to the examination. It was uncertain based on the interpretation of the radiologist whether the changes were due to extravasation of the contrast material or due to the patient's pathology.
A follow-up computed tomography scan of the pelvis was made when the patient presented. The findings were similar to those in the previous CT scan. There was more definite calcification within the substance of the muscle with a ring that like area of calcification surrounding an unclassified area.
CT scan guided aspiration of the area of the potential collection or calcified muscle was made and there was no fluid. Cultures showed no growth after five days. The radiologist performing the procedure noted that there was palpable calcification within the muscle.
A follow-up magnetic resonance imaging scan of the pelvis was made four days later, this time with no injection of contrast material. This MRI showed that the findings on the previous MRI we are due to the patient's pathology and not due to extravasation of contrast material. The findings were similar in extent to the previous MRI with no significant improvement nor any significant worsening.
Laboratory results:
When the patient presented he was afebrile. He denied any fevers at any time. On presentation, vital signs were stable.
The patient walks with a hunched forward gait pattern and has a strong limp. He cannot straighten up because extending and straightening his hip are very painful. He has difficulty with walking and daily activities.
The left groin is slightly warm. There is no definite mass. The examination does not detect any fullness or lymphadenopathy. The patient can gently move the hip. If the patient move his hip gently it does not cause pain. Any type of twisting of the hip causes extreme pain. Extending the hip and the iliopsoas cause a significant pain. There is tenderness to palpation over the left anterior inguinal ligament and along the anterior superior iliac spine on the medial side of the left lower abdomen..
ESR rate is elevated at more than 50, and his white count is elevated to 14. Creatine kinase is normal. Other labs are normal.
The patient walks with a hunched forward gait pattern and has a strong limp. He cannot straighten up because extending and straightening his hip are very painful. He has difficulty with walking and daily activities.
The left groin is slightly warm. There is no definite mass. The examination does not detect any fullness or lymphadenopathy. The patient can gently move the hip. If the patient move his hip gently it does not cause pain. Any type of twisting of the hip causes extreme pain. Extending the hip and the iliopsoas cause a significant pain. There is tenderness to palpation over the left anterior inguinal ligament and along the anterior superior iliac spine on the medial side of the left lower abdomen..
ESR rate is elevated at more than 50, and his white count is elevated to 14. Creatine kinase is normal. Other labs are normal.
Differential Diagnosis
These findings are consistent with sarcoma, infection, or myositis ossificans circumscripta.
Further Work Up Needed:
follow-up is necessary to determine the amount of calcification and the appropriate treatment of the calcification.
Pathology results:
no biopsy was performed. Based on the clinical evolution of the patient and response to treatment, it did not appear to be necessary to biopsy the lesion to confirm the diagnosis.
Treatment Options:
treatment of this is detailed in the myositis ossificans page on this website. Of interest: This patient states that marijuana use was very helpful in relieving his pain while conventional pain medications were not effective.
Special Features of this Case:
This 42 year old healthy man presented with insidious onset of left groin and hip pain, which worsened to the point where could not walk and required strong narcotic pain medications. The pain got so severe he was admitted to the hospital for tests and treatments. No diagnosis could be made by the doctors and the pain got worse. The patient decided to go home and go to a different doctor.
The patient had very dramatic changes on MRI scan and on CT scan with subtle peripheral calcification of the area of maximum abnormality and tenderness. On a follow-up CT scan the calcification had become more pronounced and more easily visible, and could be seen to have a peripheral or zonal pattern that is consistent with myositis ossificans circumscripta.
Myositis ossificans circumscripta is difficult to distinguish from malignancy and infection. It can mimic infiltrative malignancies and tumors. Please refer to the myositis ossificans page on this website for further information on this unusual tumor mimic.
The findings were consistent with infection, particularly a psoas abscess or pelvic abscess. The patient was never febrile during his illness. Although the patient had an elevated sedimentation rate and elevated white cell count, aspiration of the abnormal area confirmed that no infection was present.
The findings were less consistent with malignancy. The infiltrative nature of the signal abnormality in the muscle on the MRI scans is not consistent with sarcoma, which grows in a centipedal fashion and typically is well-defined with distinct borders and a visible pseudocapsule. Other types of infiltrated malignant tumors might conceivably present this way, such as lymphoma, and perhaps extraskeletal Ewing sarcoma.
The patient had very dramatic changes on MRI scan and on CT scan with subtle peripheral calcification of the area of maximum abnormality and tenderness. On a follow-up CT scan the calcification had become more pronounced and more easily visible, and could be seen to have a peripheral or zonal pattern that is consistent with myositis ossificans circumscripta.
Myositis ossificans circumscripta is difficult to distinguish from malignancy and infection. It can mimic infiltrative malignancies and tumors. Please refer to the myositis ossificans page on this website for further information on this unusual tumor mimic.
The findings were consistent with infection, particularly a psoas abscess or pelvic abscess. The patient was never febrile during his illness. Although the patient had an elevated sedimentation rate and elevated white cell count, aspiration of the abnormal area confirmed that no infection was present.
The findings were less consistent with malignancy. The infiltrative nature of the signal abnormality in the muscle on the MRI scans is not consistent with sarcoma, which grows in a centipedal fashion and typically is well-defined with distinct borders and a visible pseudocapsule. Other types of infiltrated malignant tumors might conceivably present this way, such as lymphoma, and perhaps extraskeletal Ewing sarcoma.
Imagen
Case ID Number
Image Types
Image modality
Tumor Name
Example Image
yes
Tumor Type
Benign or Malignant
Body region








