Case Identification
Case ID Number
Tumor Type
Body region
Position within the bone
Periosteal reaction
Benign or Malignant
Clinical case information
Case presentation
This delightful 90-year-old woman has pain in the right foot, in the midfoot at the base of the second and third metatarsals. There is a lesion on the x-rays and on the MRI in that area. The patient has a history of nephrectomy for renal cell carcinoma 6 years ago.
Radiological findings:
On the plain radiographs, there is a lytic, destructive, completely lucent lesion in the base of the second metatarsal, that seems to extend in into the base of the third metatarsal. There may be very faint mineralization of the lesion. Deletion has a relatively aggressive appearance. There is no periosteal reaction present. There is diffuse demineralization of the nearby bones.
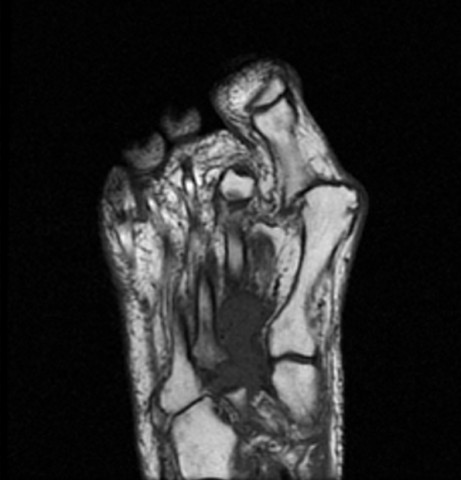
An MRI shows a T1 dark, T2 intermediate lesion extending across the second and third metatarsal base, into the base of the cuneiforms. It has a slightly lobular outline that extends outside the contour of the bones themselves.
An MRI shows a T1 dark, T2 intermediate lesion extending across the second and third metatarsal base, into the base of the cuneiforms. It has a slightly lobular outline that extends outside the contour of the bones themselves.
Laboratory results:
no laboratory examinations are requested
Differential Diagnosis
The working diagnosis would be metastasis from renal cell carcinoma. Other metastasis such as from lung and breast carcinoma is possible. Although metastatic deposits in the bones of the foot are rare, they definitely can occur, and should be at the top of the differential in a patient with a prior history of cancer with propensity to metastasize to bone and the new onset of foot pain with a bone lesion.
Further Work Up Needed:
The patient needs a complete assessment of the skeleton, including a whole body bone scan, and a CT scan of the chest, abdomen, and pelvis with oral and intravenous contrast. This workup combined with the x-rays and MRI of the foot, will complete the radiological examinations necessary to stage the patient. The biopsy will provide the histological information necessary to confirm the local lesion, and the slides and blocks from the original nephrectomy should be reexamined to compare these with the cells from the foot. Together, this series of procedures will confirm the diagnosis, the stage of the disease, and these two pieces of information lead directly to the preferred treatment.
Pathology results:
See the images from the frozen section that are shown. Findings include abundant foamy and in some areas clear cytoplasm, round nuclei with prominent nucleoli, and prominent small blood vessels in the tumor. Final analysis is pending.
Treatment Options:
Patients with metastatic lesions in the foot require surgical treatment for biopsy only. It is uncommon that reconstructive surgical intervention is necessary. Radiation treatment is mandatory, and bisphosphonate medication such as Zometa should be given as soon as the patient can receive them to prevent further bone damage as much as possible. In most of these cases, the patient is immobilized in a removable walking boot and allow to be partially weightbearing.
Special Features of this Case:
Although uncommon, a presentation of metastatic carcinoma with deposits in the skeleton of the foot can occur. A number of case reports of presentation of renal cell carcinoma with metastasis to the foot have been published.
Foot Ankle Spec. 2008 Dec;1(6):338-43. Epub 2008 Oct 21.
Metastases to bones of the foot: a case series, review of the literature, and a systematic approach to diagnosis.
El Ghazaly SA, DeGroot H 3rd.
Foot Ankle Spec. 2008 Dec;1(6):338-43. Epub 2008 Oct 21.
Metastases to bones of the foot: a case series, review of the literature, and a systematic approach to diagnosis.
El Ghazaly SA, DeGroot H 3rd.
Image
Secret Tumor Name
Case ID Number
Image Types
Image modality
Tumor Name
Tumor Type
Benign or Malignant
Body region
Bone name








