Summary
Description
This solitary lesion has a predilection for the bones of the hands and feet, facial bones, skull, and jaw. It is a non-neoplastic, reactive lesion of unknown etiology.
People and Age
All ages are affected.
Symptoms and Presentation
Pain and swelling are common symptoms. There is usually no distinct mass.
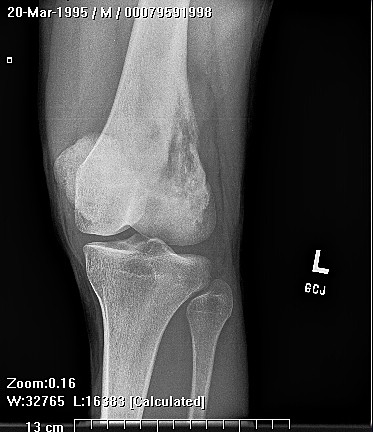
Brief description of the xray
The lesion is lytic, actively destroying bone, it may thin or destroy the nearby cortex, but no perisosteal reaction is seen.
Brief desc of tx
Intralesional curettage and bone grafting are sufficient.
Tumor Name
Tumor Type
Benign or Malignant
Most Common Bones
Location in bone
Periosteal reaction
Position within the bone
Tumor behavior
Tumor density
Complete Information on this Tumor
Introduction and Definition
This solitary lesion has a predilection for the bones of the hands and feet, facial bones, skull, and jaw. It is a non-neoplastic, reactive lesion of unknown etiology. It may be due to injury, trauma, or intraosseous hemmorhage. The name "solid variant of aneurysmal bone cyst" is also given to this tumor.
Incidence and Demographics
The age range is from childhood to older adults. There does not appear to be a definite age of peak incidence for this lesion. Most cases are in the jaw, facial bones, and skull, short bones of the hands and feet, and a few cases have been reported in the long bones of the upper and lower extremities.
Symptoms and Presentation
Pain and swelling, or a slight pathological fracture
X-Ray Appearance and Advanced Imaging Findings
The lesion is lytic, slightly expansile, actively destroying bone, it may thin or destroy the nearby cortex, but no perisosteal reaction is seen. The lesion does not seem capable of forming an extraosseous mass. The borders may be indistinct, and the lesion may have a slightly aggressive appearance. The location within the bone is variable, and may even be subperiosteal. In the author's series, no overlying thin layer of reactive bone is seen covering the extraosseous portion of the tumor, which may be present in GCT and ABC's. There is no mineralization of the matrix. These lesions cannot be readily distinguished from other active, lytic processes such as ABC, GCT, or primary sarcoma, or metastatic cancer.
Laboratory Findings
No diagnostic lab findings exist., but labs may be useful to eliminate other tumors in the differential.
Differential Diagnosis
ABC, GCT, brown tumor, metastasis, infection. The appearance of the lesion may be aggressive.
Preferred Biopsy Technique for this Tumor
open
Histopathology findings
The microscopic findings are shown. There is reactive granulation tissue, spindle-shaped fibroblasts, focal hemorrhage, and scattered small giant cells that have few nuclei. The giant cells may cluster around areas of hemorrhage. Irregular bony trabeculae have osteoclastic giant cells on some surfaces. Some cases have had much more frequent giant cells.
Treatment Options for this Tumor
Curettage, with bone graft or other bone void filler to treat the bone defect.
Preferred Margin for this Tumor
intralesional
Outcomes of Treatment and Prognosis
Recurrence is not common.
Special and Unusual Features
The presence of giant cells leads to the potential for confusion with ABC, GCT, PVNS, and brown tumor.
Suggested Reading and Reference
Giant-cell reparative granuloma of the hand and foot bones
Ratner-V; Dorfman-HD Department of Orthopaedic Surgery, Montefiore Medical Center, Bronx, New York 10467-2490. Clin-Orthop. 1990 Nov(260): 251-8
Ratner-V; Dorfman-HD Department of Orthopaedic Surgery, Montefiore Medical Center, Bronx, New York 10467-2490. Clin-Orthop. 1990 Nov(260): 251-8